GoalAt the completion of this module, the participant will be able to identify developmental issues specific to LGBT people across the lifespan. ObjectivesThe reader should be able to demonstrate
Pre-Test
|
| The one prospective, longitudinal study of boys with extreme gender atypical behavior ("sissy boys") found that 75 percent of these boys reported homosexual orientation as adolescents and young adults (Green 1987). Only one declared himself to be transsexual in adolescence. These subjects are not necessarily representative of all boys (let alone girls) who will grow up to be homosexual adults. However, it is clear that gender atypical children face varying degrees of hostility and homophobia from their families, peers, and even some mental health professionals. This hostility takes the form of marginalization, teasing, insults, assaults, and sexual violence. These in turn lead to feelings of shame, anxiety, depression, and poor self-esteem in the affected child. Some may actively and self-consciously struggle to alter their behavior to conform to peer expectations, cultural norms, and religious values. This can lead to a deeply engrained internalized homophobia manifested as profound self-hatred, as well as externalized as anti-gay attitudes and aggression in adolescence and young adulthood. This aggressive suppression of this forbidden part of themselves can lead in later life to desperate attempts at heterosexual relations, marriage and child rearing, while maintaining a secret life of homosexual activity. The presence of gender variance, interests and behaviors more typical of the opposite does not necessarily imply gender identity disturbance. Relatively few boys with gender variance will become transgender adults and most will later become gay adults. Parents with a gender variant child can be encouraged to help their child feel secure about their gender identity while minimizing ostracism and isolation. Child psychiatrists can provide treatment for any resulting distress or behavioral disorders and help parents discuss what it may be like to have a gay or lesbian child (Perrin 2004). |
Harvey Fierstein's The Sissy Duckling |
Sexual Identity Development in AdolescenceSexual exploration and experimentation are common in adolescence. Many heterosexual youth have sexual experiences with persons of the same sex, and many homosexual youth with persons of the opposite sex . For straight youth, this may represent curiosity and experimentation, while lesbian and gay youth may be experiencing pressure to conform to majority behavior. Adolescent development in LGB youth is often conceptualized using stage models that include phases of identity development such as awareness of difference, confusion about difference, decision and action (or indecision and inaction), acceptance, pride, and integration. However, these developmental have often been based on retrospective accounts of adults rather than prospective studies. Stage conceptions of sexual orientation development may not fully capture the messiness of real life with its overlaps, missing steps, and stages occurring out of order. Nonetheless, studies of LGBT young adults show that most recognized their sexual orientation during early adolescence, with awareness of same-sex erotic attraction usually predating puberty (Cohler 2000). [See also the Identity and Coming Out sections] Coming out may be different for today's LGBT youth than it was for past generations. For some LGBT youth, expectations of stigma may be absent, and some aspects of LGBT life may even be considered "cool." Most adolescents with same-sex attractions do not identify as LGBT or have same sex-behaviors while adolescents, and some may consider labels such as "gay" or "lesbian" too constraining, calling themselves "queer" or rejecting all labels. Nonetheless, studies of LGBT young adults show that most recognized their sexual orientation during early adolescence, with awareness of same-sex erotic attraction usually predating puberty. Stress Factors Influencing LGBT Adolescent DevelopmentLGBT adolescents have the same basic needs as other youth: development of self-esteem, identity, and intimacy; social and emotional well-being; and physical health. LGBT adolescents may be especially vulnerable to not having their basic needs met. They may feel different from their peers, and unsure how their friends and family will react to their sexual orientation. They often lack other outlets for exploring their sexual identity, such as talking to mentors or same-sex dating. LGBT adolescents are subject to high rates of physical and verbal abuse, being forced out of their homes, and sexual assault. Although most LGBT youth show remarkable resilience, these factors combined with stigma may be related to higher rates found in LGBT adolescents of dropping out of school, using tobacco, alcohol or drugs, suicide attempts, depression, and HIV disease (Frankowski 2004). Physicians and LGBT AdolescentsPhysicians, especially pediatricians and child psychiatrists, have an important role to play in addressing the development concerns of LGBT adolescents. It is essential that they strive to be open and inclusive in their interviewing and responses to questions from patients. For instance, rather than just asking whether a young girl has a boyfriend, she can be asked whether she has ever had a romantic relationship with a boy or girl . It is important to explore multiple aspects of sexual identity, including sexual attraction, self-labelling, and sexual behaviors. Confidentiality is essential, both to encourage openness and also because many LGBT youth have home environments that might become dangerous if their sexual orientation is revealed. Clinicians should incorporate in their treatment of LGBT patients questions about available supports, HIV risk factors, physical and sexual abuse, drug and alcohol use, and suicidality. Referrals to psychotherapy should be considered to help teens clarify and become more comfortable with their sexual orientation and adjust to resulting issues and conflicts (Frankowski 2004). Referrals to LGBT resources such as gay-straight alliances at school (www.glsen.org) or The National Coalition for Gay, Lesbian, Bisexual and Transgender Youth (www.outproud.org). Parent education may be essential, with the permission of the LGBT adolescent, and resources such as PFLAG (www.pflag.org) are available. |
|
IdentitySexuality and sexual identities can be diverse and complex. Kinsey (1948, 1953) exposed some of this diversity with the development of the Kinsey scale. The scale goes from 0, totally heterosexual, to 6, totally homosexual. Adding to the Kinsey scale is the idea of dimensions of sexuality (Klein et. al., 1985), an acknowledgement that people can not only fall between the 0 and 6 poles, but that they can rate differently with respect to sexual attraction, with whom they fall in love, and sexual behavior. Identity adds yet another dimension, so that a person with bisexual behavior (having sexual relations with both men and women) may self-identify as bisexual, gay, or straight. Some have suggested that a one-dimensional scale is too simplistic, because it necessarily implies that if someone is more attracted to one gender, he or she is less attracted to the other. A two-dimensional scale would account for people who feel 100% attracted to both genders, as well as people who feel very little attraction toward either gender (asexual). Scales like Kinsey are generally not practical for describing one’s own identity. People need to have a coherent and consistent identity and life story, so ultimately tend to put themselves into categories of straight, gay, or bisexual, rather than describing themselves as “a 3” or “a 5 on attraction, a 4 on behavior.” Moreover, homosexual feelings and behavior are subject to stigma and discrimination, so to acknowledge homosexual feelings and adopt an identity that is bisexual or gay usually means that the person has strong and predominant same-sex attraction. Still, some people, perhaps women more than men, have adopted a myriad of terms to describe different shades of identity: gay, lesbian, bisexual, bi-dyke, queer, and others. |
|
Coming OutComing out is the process of becoming aware of and acknowledging one’s own gay identity (coming out to oneself), and disclosing that identity to others (coming out to others). It is a developmental process unique to gay people. The concepts of coming out and gay identities are relatively new ones (see History module). Coming out to oneselfAwareness and development of a gay, lesbian, or bisexual (GLB) identity is not a single event, but a process, usually a lifelong process that parallels one’s development as a person. Coming out to oneself encompasses events such as awareness of a first same-sex attraction or crush, first same-sex kiss, feelings of being “different” from peers as a child or adolescent, self-questioning (“Am I gay?”), the first experience of going to a gay bar or gay pride parade, self-labeling (“I am gay”), and many other events in a person’s life. Coming out often starts in young adulthood, but can begin at any age or stage of life. Acknowledging, acting on, and integrating same-sex feelings into one’s identity can be an exhilarating and terrifying process. Coming out can be accompanied by mood swings and impulsivity, much like a second adolescence, and might lead to an erroneous diagnosis of borderline personality disorder by an uninformed clinician. Cass (1979, 1984) has described stages of homosexual identity formation, from identity confusion to acceptance and pride, which could be considered stages of coming out. While this provides some helpful framework, it must be noted that the process of coming out is often not linear, and individual gay people may not fit neatly into such models. |
|
Not every person who becomes aware of same-sex attractions or desire ends up identifying as GLB. The person may accept or reject such feelings, and accordingly adopt a GLB identity or not . Over time, a person may become more or less accepting of his or her homosexual feelings and his or her sense of identity may shift. A well-intentioned therapist treating a patient who is struggling with whether he or she is GLB may be tempted to quickly push a resolution. Comments such as, “You just have to accept that you’re gay,” or, “It’s really OK to be a lesbian” may be well-meaning, but are generally not helpful to the person in the midst of an intrapsychic conflict, and may even drive the person from treatment. It is also not uncommon for an adolescent or adult questioning his or her sexuality to ask the therapist, "Do you think I’m gay?" Again, rendering an opinion on how the therapist thinks the patient will (or should) work out his or her identity is generally not a helpful intervention. (See also the Therapy module) GLB people have internalized societal views of homosexuality (internalized homophobia, heterosexism), and often retain biased thinking and stereotypes about gay people (and by extension, themselves) even after they have apparently become comfortable with their identity. New situations and relationships can bring out these retained views, sometimes precipitating an identity crisis but also allowing for the possibility of further growth and maturity. Drescher (1998) describes a gay male patient who came into treatment after his ten-year relationship had ended. The patient was a middle-aged man who had long felt comfortable with his gay identity. Yet when the relationship ended, he had the thought that it was because “gay relationships can’t last.” The end of this relationship had called into question any future relationships, and indeed his whole identity. He felt paralyzed and unable to do the practical things needed to sell the house he and his ex-partner had purchased together. When he became aware of how his internalized homophobia came into play around the breakup, the patient was able to sell his house and go on with his life. It has been generally believed that women come out to themselves at later ages then men, although the early literature did not support this (Barber 2000). More recent literature has shown that gender differences may exist, although not as simplistically as predicted. Savin-Williams & Diamond (2000) found in a group of sexual minority youth that men and women became aware of same-sex attraction at about the same age. Men were more likely to follow a “sex first” trajectory of having a sexual experience with another man and then self-labeling as gay. Women were more likely to follow a “label first” process of identifying as gay and then having a sexual experience with another woman. Some gender differences in coming out may be attributable to lesbian invisibility. Other potential factors are societal encouragement of men to express and women to suppress their sexual feelings, and differences in male and female sexuality in general. Additionally, there is known to be greater societal condemnation of cross-gender behavior in boys than girls, so that boys with cross-gender interests might be confronted by their difference at an earlier age than girls. Coming out to othersSince society assumes everyone is heterosexual (heterosexism), and since gay people do not have lavender skin or other obvious identifying characteristics, coming out to others is also a lifelong process. Everyday situations, from the critically important to the mundane, offer a gay person the decision of whether or not to disclose his or her identity. Becoming a parent, moving to a new town, changing jobs and other major life changes can open up a whole new sphere of people about whom a gay person will have to make this decision. |
(From Drescher 2004) |
BisexualityAlthough the dominant paradigm of sexuality derived from the illness model of homosexuality, splits people into two groups: homosexual and heterosexual, research on human sexuality indicates that a substantial percentage of the population feels sexual attraction to both men and women. The word bisexual is used both as an adjective to describe sexual attraction to and behavior with both sexes and as a noun to label individuals who have a bisexual sexual orientation. Bisexual people are not necessarily (and generally are not) attracted equally to men and women. The percentage of the population that feels sexual attraction to both men and women is larger than the percentage of the population that has sexual experiences with both sexes, which in turn is larger than the group that identifies as bisexual. For example, a heterosexually-married man who has sex with men is behaviorally bisexual, but may identify as straight (see down low ). Some people may view themselves as bisexual during a transitional period when they are coming out, while others may maintain a lifelong bisexual identity. Those who do identify as bisexual over time sometimes face prejudice from members of the gay community who may assume that they are uncomfortable with coming out as gay or lesbian. Gay men and lesbians may accuse bisexuals of enjoying heterosexual privilege, particularly if they are heterosexually partnered or married. However, heterosexually-partnered bisexuals face increased invisibility and isolation as people around them assume that they are straight. They may face bias from straight people who sometimes wrongly assume that being bisexual means that the person needs to have male and female partners simultaneously. Because bisexuals may not feel fully accepted by either the gay or the straight community, they may seek out other bisexuals for support (http://www.biresource.org, http://www.binetusa.org). |
 |
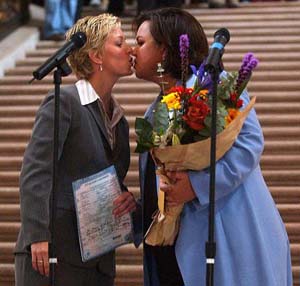
The Lesbian Couple |
 |
The Gay Male CoupleNatural History and Challenges to IntimacyIn discussing gay male couples, it is valuable to explore both how they are similar to and different from heterosexual couples. Greenan and Tunnell (2003) vividly describe the sociocultural developmental factors that affect the growing gay boy's capacity for intimate relatedness and the kinds of difficulties they see in the male couples. These challenges to intimacy often begin during the boy's childhood, precipitated by the awareness of homoerotic desire or with the emergence of gender discordant behavior, such a dislike of aggressive play or affinity for playing with dolls. These boys, destined to grow up to be gay, are subject both to the cultural demands of being male and the stigmatizing effects of secrecy about their sexual orientation, sometimes made worse by the father's frightened distancing. There is good reason for the growing gay boy to develop a mistrust of other men and an expectation that his longing for intimacy with a man will result in shame and rejection, as this is often the case with his father. Within the family, there is often a powerful admonition to keep his erotic feelings a deep and extremely well guarded secret. He learns that the expression of these persistent feelings will threaten much-needed affectionate ties to parents, friends, and siblings. Therefore a false self, pseudo-heterosexual or asexual, is created with the suppression of his erotic and affectionate yearnings for other men. This is often accompanied by a more global suppression of genuine affect of all kinds in the service of passing as a "normal" boy with deep emotion well hidden. The discovery of erotic feelings is traumatic for the gay boy in ways that it is not for straight boys who are allowed to speak of and even explore their heterosexual desires. For the gay boy, the development of an identity as a sexual/affectionate being is surrounded by admonitions of silence, threat of abandonment and isolation, and self-negation. This can be particularly painful if the boy's father senses his son's developing erotic attraction and responds with anxiety and emotional distance, which can reinforce the boy's shame and isolation. The protogay boy is left on his own with an enormous secret which cannot be shared, and this can lead to the defensive self reliance and isolation that give rise to difficulty in romantic relationships later in life. This deepens the sense that homoerotic attachment is dangerous and toxic. The absence of a supportive context in which to express desire and practice genuine relatedness in childhood can cast a long shadow into adulthood, with important ramifications for understanding and treating the difficulties that gay male couples bring into the therapist's office. McWhirter and Mattison (1984) interviewed 156 gay male couples who had been together anywhere from 2 to 37 years. They conducted both structured and semi-structured (open ended questions) interviews and organized their findings by describing six stages of development for gay male couples:
McWhirter's and Mattison's analysis normalizes gay male relationship development by emphasizing its similarities to that of heterosexual couples . Subsequent studies often discuss the differences between gay male couples and the heterosexual norm. Today, gay male couples face many choices on many issues, including: monogamy vs. the negotiation of non-monogamy, the question of raising a family, the dynamic around HIV and the negotiation of non-traditional gender roles. Many gay male couples have found sex outside the primary relationship to be a valuable and even necessary component of survival of the couple. Others find monogamy to be vital. Surrogacy and adoption have allowed gay male couples to raise children, thus creating a new model for a family and questioning traditional concepts of family and family values. The current debate over gay marriage is only one aspect of the emergence of gay relationships into the public awareness, challenging the silence and stigmatization that was discussed above. Gay relationships, as gay people, continue to act as paradoxical antipodes, both reflecting and challenging norms of gender, sexuality, family, and the concept of normality itself. |
|
Parenting
For example:
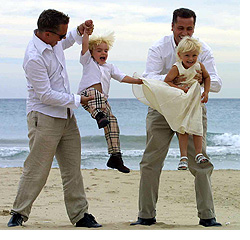
Same sex parents face many of the same challenges as straight parents, but there are some unique issues. Where one parent is the biological parent of the child or children, there can sometimes be tension if the bio parent uses her or his status to exert power in the relationship, or if the second parent feels lower in status. Same sex parents solve the issues of what the children will call them in different ways, with some using "mommy and mama" or "daddy and papa," others using names for mom or dad that reflect their heritage or ethnicity, and others having their children call them by their first names. The issues of coming out to one's kids is more pertinent for parents who first raised children in the context of a heterosexual relationship, since children raised by a same sex couple from the beginning are generally aware of their parents' relationship. Same sex couples may find that they have to come out to pediatricians, teachers, day care providers, and others who have contact with their children so that they can both share decision-making and childcare responsibilities. Same sex parents have faced legal discrimination in trying to have and raise children. In some states, gay people are banned from adopting children, while in many other states, gay couples able to adopt as a couple, not being able to give their children some of the protections that being a married couple would afford. The spouse who leaves a marriage after acknowledging that he or she is gay can face similar discrimination in decisions about custody and visitation of children from that marriage. The Academy of Pediatrics and American Psychiatric Association have both issued position statements supporting adoption and co-parenting by same sex couples, recognizing that legal support for these families will lead to healthier families and children. Having children can be fulfilling, exhausting, rewarding for same sex parents just as for heterosexual parents. It can also feel alienating to the couple, who may not have gay friends with children and who may not easily be able to participate in activities in the gay community once they have kids. They may similarly feel isolated at times in the typical parent circles as the only same-sex couple. Finding supports can be important both for the parents and kids. For gay and lesbian couples who came of age at a time when gay parenting was unheard of, or gay and lesbian couples who choose not to have children, many have nonetheless taken on a parenting role in other ways. These include being involved "aunties" and "uncles" to children of their siblings or friends, and doting on pets as if they were children. Resources deHaan, Linda and Nijland, Stern. King and King and Family. Tricycle Press, 2004. Parnell, Peter and Richardson, Justin. 2005. And Tango Makes Three. New York: Simon and Schuster. Martin, April. 1993. The Lesbian and Gay Parenting Handbook: Creating and Raising our Families. New York: Perennial. COLAGE - Children of lesbians and gays everywhere. Sponsors Family Week in Provincetown and other events. |
|
Aging |
|
Clinical ExamplesComing OutRaphael, a gay man, is at the checkout of a supermarket, buying among other items a bouquet of flowers for his partner. The woman at the register remarks, “Your wife is so lucky to have you!” Raphael may choose to challenge the checkout person’s assumptions and come out to her (“Actually I’m buying these for my partner Steve”) or may say nothing. The decision may hinge on what sort of day he’s had, his level of fatigue, how rushed he is, how safe a disclosure of a male partner might be in his town, and other factors. Pamela, a lesbian who has a three-year old child with her partner is alone registering the child for admission to a daycare center. The center’s director has her fill out a form, which has a space for “mother” and “father.” Here the decision has greater consequences, in that if Pamela chooses not to put her partner’s name on the form, her partner will not be able to pick up the child or respond to the child in an emergency. On the other hand, Pamela may fear that the daycare will not accept her child for admission if the director knows she has lesbian parents, or that staff at the daycare will treat her child differently. These factors may be more or less important depending on the area in which they live, the scarcity of daycare slots, Pamela’s and her partner’s role in taking care of their child, and other issues. Gay male couplesCommon issues emerged in the course of the treatment of a couple that presented for help in deciding whether to remain together or part ways. Andrew came from a wealthy, intellectually rich family setting, but grew up with narcissistic parents who were acutely aware of social norms and appearances. Brian grew up in a working class family, the oldest son of a young single mother. Andrew was younger, but had had many short-term relationships; Brian had had only one major relationship, which ended with the death of his partner from cancer. Andrew felt a deep sense of safety and protectiveness in the warmth of Brian's stability and abiding love, but wanted to have sexual exploration outside the relationship. Brian was able to accept this, but with reservation and some fearfulness about the impact of this on their future. Andrew wanted Brian to be less fearful and even to join him in sexual exploration outside of the relationship, but Brian did not want to do this. Andrew repeatedly felt that Brian was interested in the appearance of a closed, monogamous relationship and feared being trapped in a situation that was defined by social convention, just like the relationship he grew up in. At an unconscious level, though, Brian's deep love for him made Andrew anxious and suspicious. It felt threatening and "glommy." The exuberance of sexual variety helped him feel masculine and sexy. Brian felt hurt that his love was experienced as feminizing or stifling, when he was well aware of Andrew's hunger and dependence on it for security and safety. Brian on the other hand suffered from very intense father hunger, having grown up without one. Since he had already been a father figure to his younger siblings, he readily took on this role with Andrew while maintaining his own hunger to be cared for as very secret and shameful. In fact, Andrew enacted some of Brian's worst fears about his own father (difficulty with commitment and faithfulness) and evoked some of Brian's deepest fears (abandonment by a man he loved). The therapy for this couple focused on the elucidation of these patterns, working through of transferences to each other. With this, they were better able to understand their relationship and to find new ways to meet each others' needs. Post-Test
References |
|